Few questions cause more anxiety among Essential Tremor patients than this one: Will my ET eventually become Parkinson’s disease? The concern is understandable. Both conditions involve tremor, both are progressive, and both are neurological. When Essential Tremor worsens — as it does over time in most patients — the fear that something more serious is developing sits quietly in the background of every appointment and every new symptom.
The short answer is that Essential Tremor does not convert into Parkinson’s disease. They are distinct neurological conditions with different mechanisms, different circuits, and different cellular pathologies. But the relationship between them is more nuanced than a simple “no,” and that nuance is worth understanding clearly.
Two Distinct Conditions, Two Distinct Circuits
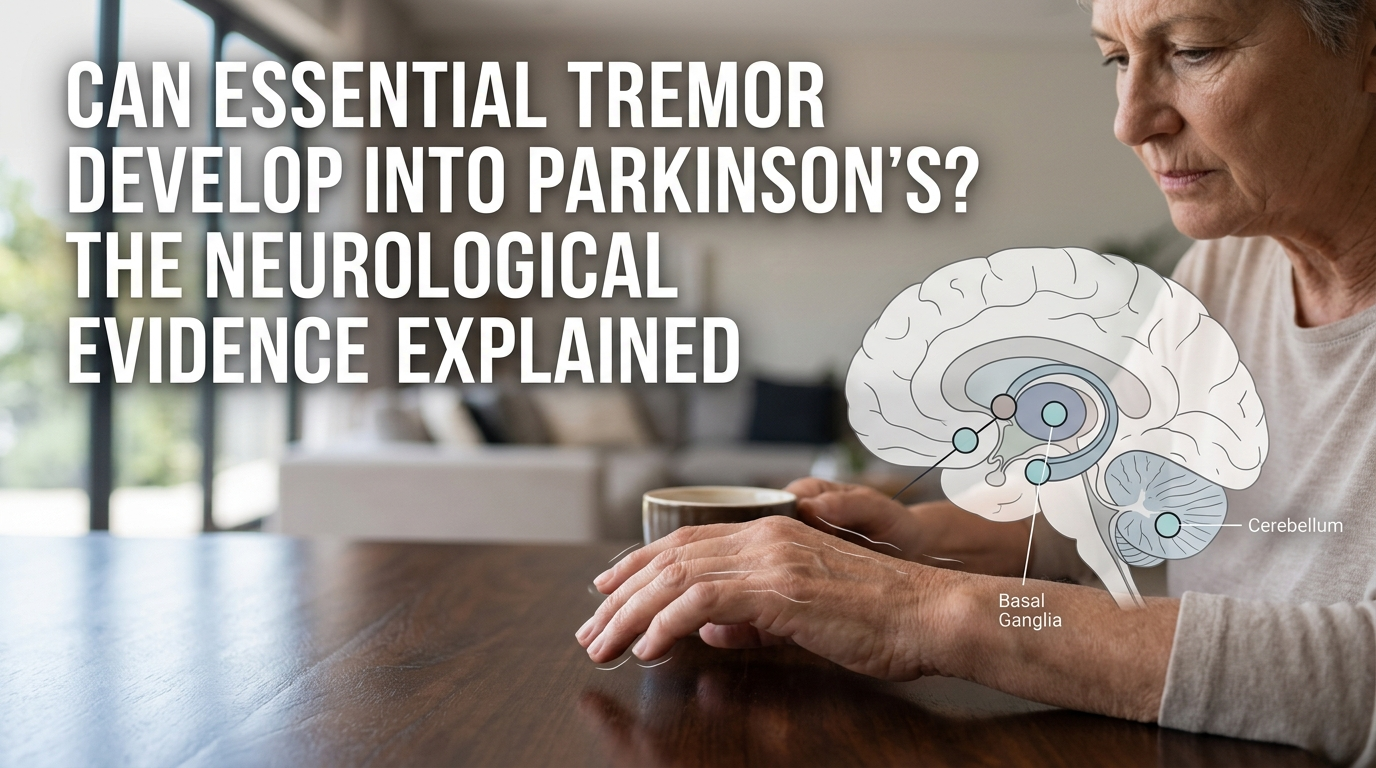
Essential Tremor is an action tremor — it appears during voluntary movement and is driven by abnormal oscillatory firing in the cerebello-thalamo-cortical circuit. The cerebellum is the primary site of dysfunction. There is no significant loss of dopamine-producing neurons, and the condition does not involve the basal ganglia as Parkinson’s does.
Parkinson’s disease is fundamentally different at the cellular level. It results from the progressive death of dopamine-producing neurons in the substantia nigra, a structure within the basal ganglia. The hallmark tremor is a resting tremor — present when the hand is still, not during movement — and it’s accompanied by bradykinesia (slowness), rigidity, and postural instability. These motor features reflect a dopaminergic deficit rather than a cerebellar oscillation.
The tremors look different, originate in different brain regions, and respond to different treatments. Essential Tremor responds to alcohol, propranolol, and primidone. Parkinson’s tremor responds to levodopa and dopamine agonists. A movement disorder neurologist can usually distinguish the two on clinical examination alone.
Why the Confusion Exists
Several factors feed the misconception that ET can become Parkinson’s. First, both conditions become more common with age, so it’s statistically possible — though uncommon — for a person to develop both independently. When a patient with longstanding ET develops new Parkinson’s symptoms in their 70s, it can look like one condition “turned into” the other. In reality, a second, unrelated condition has appeared.
Second, Essential Tremor can develop features over time that superficially resemble Parkinson’s. Some long-duration ET patients develop mild gait changes, slight balance issues, or cognitive slowing. These are now understood to be part of the ET spectrum in advanced cases, rather than early Parkinson’s. The ET Plus classification, introduced by the Movement Disorder Society, was designed to describe ET patients who develop these additional features without meeting the criteria for Parkinson’s disease.
Third, misdiagnosis runs in both directions. Studies have found that a meaningful percentage of patients initially diagnosed with ET are later reclassified as Parkinson’s — not because ET converted, but because the initial diagnosis was incorrect. Resting tremor can be subtle in early Parkinson’s, and some patients present with what appears to be an action tremor before other cardinal signs emerge.
What the Research Actually Shows
Population-level studies have found that people with Essential Tremor may have a modestly elevated risk of developing Parkinson’s disease compared to the general population, roughly 2 to 4 times higher in some cohorts. But context matters. The absolute risk remains low. Most ET patients will never develop Parkinson’s. And it remains unclear whether the association is causal, coincidental (both conditions increase with age), or an artifact of diagnostic overlap and misclassification.
No study has demonstrated a biological mechanism by which Essential Tremor transforms into Parkinson’s disease. The cerebellar pathology of ET does not progress into the basal ganglia pathology of Parkinson’s. They are not on the same neurological continuum.
When to Raise the Question With Your Neurologist
Worsening tremor alone is not a reason to suspect Parkinson’s. Essential Tremor is progressive — it gets worse over the years in most patients, and that worsening is part of the condition, not evidence of conversion.
The signs that warrant a fresh evaluation are the ones that fall outside the ET pattern entirely: a new resting tremor that appears when the hand is completely still, rigidity or stiffness in the limbs that isn’t explained by arthritis or musculoskeletal issues, a noticeable slowing of movement (buttoning a shirt takes longer, facial expressions flatten), reduced arm swing on one side while walking, or a shuffling gait. Any of these, especially in combination, warrants evaluation by a movement disorder specialist — not a general neurologist and not a general practitioner.
Managing Tremor Across Both Conditions With Steadiwear
Whether you’re managing Essential Tremor, navigating an uncertain diagnosis, or living with both conditions simultaneously, the daily challenge is the same: hand tremor interferes with eating, writing, drinking, and the tasks that define independence. Our Steadi-3 was designed for exactly this overlap.
It’s a battery-free, wearable tremor stabilizer that uses magnetically tuned mass damper technology to mechanically counteract tremor motion — regardless of whether the tremor originates in the cerebellum or the basal ganglia. Clinically validated with 85% tremor reduction and FDA Class I registered, it works for both Essential Tremor and Parkinson’s tremor without medication, without a prescription, and without needing a confirmed diagnosis to start using it.
Conclusion
Essential Tremor does not turn into Parkinson’s disease. They are neurologically distinct conditions that affect different brain circuits and different neurotransmitter systems. The confusion is understandable — both involve tremor, both progress, and both become more common with age — but the evidence is clear: one does not become the other. If your ET is worsening, that’s expected. If new symptoms outside the tremor pattern appear, that’s when a specialist evaluation matters. And regardless of the diagnosis, the daily management of tremor is a problem that has practical, immediate solutions.